This section of our NREMT study guide provides a comprehensive overview of the essential knowledge required for the Trauma component of the NREMT exam.
It covers patient assessment, management of life threatening injuries, specific injury types by body system, and environmental trauma.
Initial Patient Assessment and Management
The Rapid Trauma Exam
The rapid trauma exam is a quick, systematic assessment to identify all life threatening injuries. This head to toe survey should take no more than 90 seconds. A common mnemonic used during the exam is DCAP BTLS:
- Deformities
- Contusions
- Abrasions
- Punctures / Penetrations
- Burns
- Tenderness
- Lacerations
- Swelling
Glasgow Coma Scale (GCS)
The Glasgow Coma Scale is a standardized tool used to assess a patient’s level of consciousness by evaluating their eye, verbal, and motor responses. The total score ranges from 3 (completely unresponsive) to 15 (fully alert and oriented). A lower score indicates a more severe impairment of consciousness.
The score is calculated by adding the points from each of the three categories:
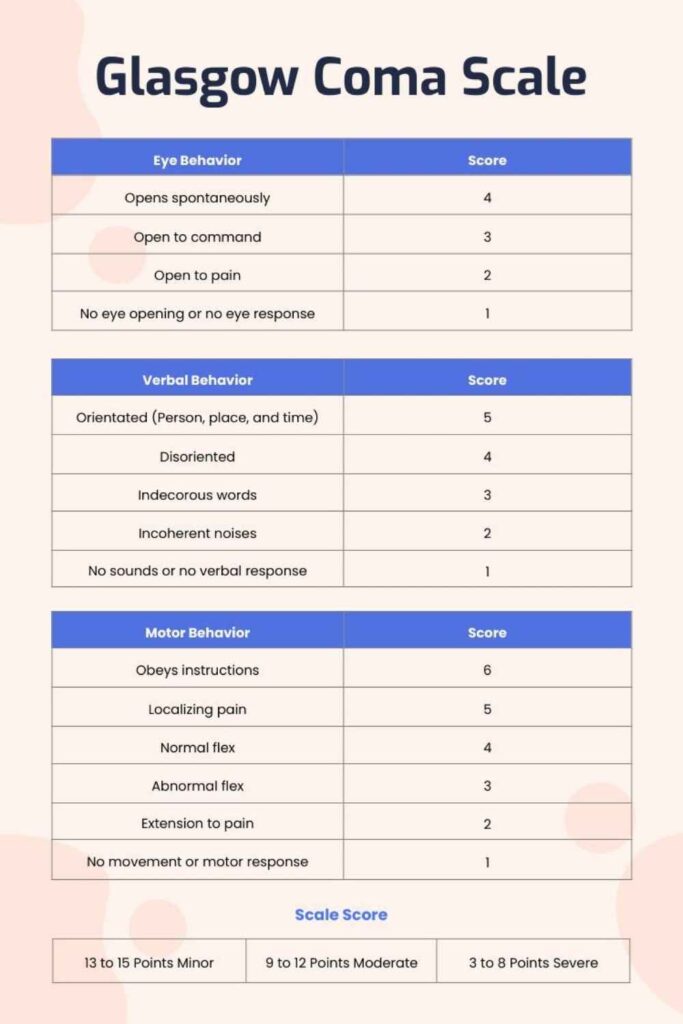
1. Eye Opening Response (E)
- 4 Points: Spontaneous (opens eyes without stimulation)
- 3 Points: To Speech (opens eyes to verbal command)
- 2 Points: To Pain (opens eyes to a painful stimulus)
- 1 Point: No Response
2. Verbal Response (V)
- 5 Points: Oriented (knows person, place, time, and event)
- 4 Points: Confused (answers questions but is disoriented in some way)
- 3 Points: Inappropriate Words (says logical words, but they are random and not in context)
- 2 Points: Incomprehensible Sounds (makes sounds like moaning or groaning, but no understandable words)
- 1 Point: No Response
3. Motor Response (M)
- 6 Points: Obeys Commands (can perform simple tasks when asked)
- 5 Points: Localizes Pain (purposefully moves to remove a painful stimulus)
- 4 Points: Withdraws from Pain (pulls away from a painful stimulus)
- 3 Points: Abnormal Flexion (Decorticate posturing; flexes arms toward the core)
- 2 Points: Abnormal Extension (Decerebrate posturing; extends arms and legs stiffly)
- 1 Point: No Response
Scoring Interpretation:
- Total Score = E + V + M
- Mild Head Injury: GCS 13–15
- Moderate Head Injury: GCS 9–12
- Severe Head Injury: GCS 3–8 (A GCS of 8 or less typically indicates a severe injury and the need for advanced airway management).
Prioritizing Interventions
The initial assessment focuses on immediate life threats.
- In cases of life threatening external bleeding, controlling the hemorrhage takes priority over airway and breathing concerns (C ABC approach).
- If a patient is not breathing upon assessment, your immediate focus becomes providing ventilatory assistance, even if other major injuries are present.
- Elevating an extremity to control bleeding is a controversial technique and should only be performed if there are no impaled objects, un splinted fractures, or risk to other wounds.
Head and Spine Trauma
Spinal Injury and Motion Restriction
Motion restriction of the neck is imperative for any patient with a suspected spinal injury. Allowing the neck to remain unsecured may lead to further injury.
- Cervical Collar: If an appropriately sized cervical collar is unavailable, a rolled towel or sheet can be placed around the patient’s head and taped to the backboard. Continuous manual support should be provided until the patient is fully secured. An ill fitting cervical collar should not be used.
- Long Backboard: Used for spinal motion restriction for supine patients with potential trauma injuries.
- Short Backboard (Kendrick Extrication Device): Can be used to extricate a seated patient with a suspected spinal injury before they are placed on a long backboard.
- Whiplash Injuries: These occur when a patient’s body is propelled forward while their head and neck are left behind, commonly in rear end impacts when a headrest is not properly positioned.
Helmet Removal
A helmet should only be removed if:
- It is a full face helmet.
- It allows for excessive head movement inside the helmet.
- It makes airway management or assessment difficult.
- It prevents adequate spinal motion restriction.
- The patient is in cardiac arrest.
Head Injuries
- Increased Intracranial Pressure (ICP): Signs include a unilaterally fixed and dilated pupil, abnormal respirations (such as ataxic respirations), bradycardia, and a widening pulse pressure (increasing systolic, decreasing diastolic).
- Basilar Skull Fracture: A high energy head trauma. In addition to general head injury signs, look for specific indicators: Cerebrospinal Fluid (CSF) draining from the ears, Raccoon Eyes (ecchymosis under the eyes), and Battle’s Sign (ecchymosis behind one ear).
- Epidural Hematoma: Bleeding below the skull but above the dura mater, typically from an arterial bleed. It causes a rapid increase in intracranial pressure. The patient may experience a brief loss of consciousness, wake up and seem lucid, and then lose consciousness again.
- Subdural Hematoma: A rupture of the bridging veins between the dura mater and the arachnoid membrane. Onset of symptoms is often gradual, developing over 1 to 2 days after the initial injury. Symptoms include vomiting, pupillary changes, weakness, paralysis, headache, and dizziness.
- Concussion: A mild traumatic brain injury. Symptoms include a gradually improving mental status, headache, amnesia, nausea, and loss of coordination.
Shock and Bleeding
Shock (Hypoperfusion)
In a trauma patient with cool extremities and tachycardia, you must assume hemorrhagic shock until proven otherwise.
- Early Signs: Agitation, cool and clammy extremities, tachycardia.
- Late Signs: Weak or absent peripheral pulses, hypotension.
- Clinical shock is evident after a 25 30% blood volume loss, but significant volume can be lost before signs appear.
Blood Volume
- The average adult male has about 6 liters of blood; the average female has about 5 liters.
- A 10% loss is generally well tolerated, causing only mild tachycardia.
- A 20 25% loss causes the body’s compensatory mechanisms to fail, leading to hypotension and decreased cardiac output.
- A 40% loss results in marked hypotension, decreased cardiac output, and severe lactic acidemia.
Types of Bleeding
- Venous Blood: Dark red and flows steadily.
- Arterial Blood: Bright red and spurts with each heartbeat.
The Trauma Lethal Triad
This is a combination of three conditions that are often fatal in trauma patients:
- Hypothermia: Low body temperature.
- Coagulopathy: Impaired ability for the blood to clot.
- Acidosis: Buildup of acid in the blood due to poor perfusion.
Musculoskeletal Trauma
Fractures
- General Signs: Crepitus (a grinding sound or sensation), shortening of the limb, deformity, and false motion.
- Pelvic Fracture: This is a potentially fatal injury due to the risk of massive internal hemorrhage. Several liters of blood can drain into the pelvic space and retroperitoneal space. Signs include hypotension and shock. Management includes applying a pelvic binder and using a scoop stretcher or backboard.
- Femoral Shaft Fracture: Also a serious injury, with potential for 500 to 1000 mL of blood loss, leading to hypovolemic shock. Traction splints are the indicated treatment.
Dislocations
- Subluxation: An incomplete dislocation of a joint or organ.
Compartment Syndrome
This is a painful condition caused by increased pressure within a muscle compartment, which restricts blood flow and can damage muscle and nerves. It typically develops within 6 8 hours of an injury.
Splinting
- Air Splint: Can be used to stabilize injuries below the knee or below the elbow.
- Hand or Wrist: Splint the limb with the hand in a position of function, with the wrist slightly bent down and fingers moderately flexed, often by placing a soft roller bandage in the palm.
- Shoulder and Upper Arm: The sling and swathe method is used to immobilize shoulder dislocations, clavicle fractures, and humeral fractures.
Soft Tissue Injuries
- Contusion: A bruise. The dermis is intact, but there is bleeding underneath, causing ecchymosis.
- Hematoma: A collection of blood within damaged tissue or a body cavity.
- Abrasion: A wound of the superficial layer of skin (a scrape).
- Avulsion: An injury that separates layers of soft tissue, which may hang as a flap or be completely detached.
- Amputation: The severing of a body part. The amputated part should be wrapped in a sterile dressing, placed in a dry plastic bag, and kept cool.
- Evisceration: Internal organs protrude from the peritoneum. Cover the organs with sterile gauze moistened with sterile saline, then secure this with an occlusive dressing. Do not attempt to push the organs back in.
Thoracic (Chest) Trauma
Flail Chest
A flail chest occurs when three or more adjacent ribs are fractured in two or more places, causing a segment of the chest wall to move independently and paradoxically (inward on inhalation, outward on exhalation) from the rest of the chest. It causes extreme pain and difficulty breathing.
Burn Injuries
Burn Classifications by Depth
- Superficial (First Degree): Involves only the epidermis. Redness and pain.
- Partial Thickness (Second Degree): Involves the epidermis and dermis. Blistering, intense pain.
- Full Thickness (Third Degree): Extends through all skin layers. Skin may be white, leathery, or charred. Nerve endings are destroyed, so the burn itself may be painless.
Burn Severity
- Minor Burns:
- Full thickness <2% of body surface area (BSA).
- Partial thickness <15% BSA.
- Superficial <50% BSA.
- Moderate Burns:
- Full thickness 2 10% BSA.
- Partial thickness 15 30% BSA.
- Superficial >50% BSA.
- Severe Burns:
- Any full thickness burn involving the hands, feet, face, airway, or genitalia.
- Any circumferential burn.
- Full thickness >10% BSA.
- Partial thickness >30% BSA.
- Burns associated with respiratory injury or fractures.
- Any moderate burn in a child under 5 or an adult over 55 is classified as severe.
Environmental Trauma
Temperature Emergencies
- Hypothermia:
- Early Signs: Shivering, rapid breathing, redness or cyanosis of the skin, tachypnea.
- Late Signs: Loss of coordination, muscle stiffness, slowed pulses, confusion/lethargy, coma, weak pulse, dysrhythmias, bradypnea, and eventually cardiac arrest.
- Heat Exhaustion: The most common heat emergency, often caused by hypovolemia from excessive sweating.
- Signs: Dizziness, weakness, altered mental status, nausea/vomiting, headaches, muscle cramps, and thirst.
- Treatment: Move to a cool environment, rehydrate, and flush skin with water for 15 20 minutes.
High Altitude and Diving Emergencies
- High Altitude Sickness: Can lead to High Altitude Pulmonary Edema (HAPE) or High Altitude Cerebral Edema (HACE).
- Scuba Diving Emergencies: Include Arterial Gas Embolism (AGE), decompression sickness (the bends), and descent pains (the squeeze).
Eye Injuries
- Retinal Detachment: The retina is pulled away from the underlying choroid. It is typically painless but presents with an increase in floaters, flashes of light (photopsia), blurred vision, and the sensation of a curtain or veil across the field of vision.
- Cataracts: A clouding of the lens of the eye, causing difficulty distinguishing colors.
- Macular Degeneration: An irreversible loss of central vision, common in the elderly. Risk factors include smoking, obesity, and sun exposure.
Trauma Knowledge Check
Test your understanding of the key trauma concepts from this section.
1. You are assessing a trauma patient who opens their eyes only in response to a painful stimulus, makes incomprehensible sounds, and withdraws from pain. What is this patient’s Glasgow Coma Scale (GCS) score?
2. A patient involved in a motorcycle collision has lost consciousness, woken up and seemed lucid for a short period, and then rapidly lost consciousness again. This presentation is a classic sign of what type of head injury?
3. While assessing a patient with chest trauma, you observe a segment of the chest wall that moves inward during inhalation and outward during exhalation. This paradoxical motion is a hallmark sign of:
4. A trauma patient presents with cool, clammy extremities and tachycardia. According to the study guide, what condition must you assume until proven otherwise?
5. Which of the following burn injuries would be classified as SEVERE according to the provided guidelines?